Tuberculosis is a communicable disease and remains one of the leading causes of ill health and death worldwide. Until the emergence of the coronavirus disease 2019 (COVID-19) pandemic, tuberculosis was the leading cause of death from a single infectious agent, ranking above human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS).1
Tuberculosis is caused by Mycobacterium tuberculosis, which is transmitted through the air when people with pulmonary tuberculosis expel bacteria, for example by coughing. The disease most commonly affects the lungs, causing pulmonary tuberculosis, but it can also affect other organs. Most people who develop tuberculosis are adults, and the disease is more common among men than women. Nearly one-quarter of the world’s population is estimated to be infected with M. tuberculosis.2
Globally, an estimated 9.9 million people developed tuberculosis in 2020, equivalent to 127 cases per 100,000 population. Adult men accounted for 56% of all tuberculosis cases, adult women for 33%, and children for 11%.2 Africa, despite accounting for approximately 11% of the world’s population, bears a disproportionate burden of tuberculosis, with substantial variation in incidence across countries. The HIV epidemic remains an important contributor to the tuberculosis burden in many African settings.3
Despite the availability of effective anti-tuberculosis treatment, unfavourable treatment outcomes continue to occur, including treatment failure. Treatment failure is a major threat to tuberculosis control. Patients who fail treatment may remain infectious, contribute to ongoing community transmission, and have an increased risk of developing drug-resistant tuberculosis, which is more difficult and costly to treat and is associated with poorer outcomes.4
The Democratic Republic of the Congo (DRC) is among the 30 countries with the highest tuberculosis burden. In 2023, the country had an estimated population of 104,066,754 and a World Health Organization (WHO)-estimated tuberculosis incidence of approximately 316 cases per 100,000 population. The DRC ranked ninth globally and second in Africa for tuberculosis burden and was among the countries simultaneously affected by high burdens of drug-susceptible tuberculosis, drug-resistant tuberculosis, and tuberculosis/HIV coinfection. In 2023, the country reported 260,515 cases of drug-susceptible tuberculosis, including 34,757 cases among children, 13,096 cases of tuberculosis/HIV coinfection, and 1,415 cases of drug-resistant tuberculosis.5
The National Tuberculosis Control Programme of the DRC, known as the Programme National de Lutte contre la Tuberculose (PNLT), aims to ensure that all people with tuberculosis have access to diagnosis and effective treatment, with a target treatment success rate of at least 90% among notified tuberculosis patients. However, despite efforts to improve tuberculosis care, treatment failure remains a concern. The reported rate of anti-tuberculosis treatment failure in the DRC increased from 1% in 2015 to 4% in 2023.6
Studies from sub-Saharan Africa have identified several factors associated with anti-tuberculosis treatment failure, including tuberculosis/HIV coinfection, previous tuberculosis, reinfection, poor adherence, and treatment interruption.7 In Kinshasa, a previous study reported that distance from the diagnostic and treatment centre, positive sputum smear after two months of treatment, missing more than one drug-refill appointment, and failure to respect the prescribed time of medication intake were associated with initial pulmonary tuberculosis treatment failure.8
However, evidence on predictors of initial anti-tuberculosis treatment failure in the DRC remains limited. This study was therefore conducted to describe the sociodemographic characteristics of tuberculosis patients treated at the Diagnostic and Treatment Centre of Kabinda General Referral Hospital and to identify factors associated with failure of initial anti-tuberculosis treatment in this setting. The findings may inform targeted interventions to improve treatment outcomes and prevent the development of multidrug-resistant tuberculosis.
METHODS
Study setting
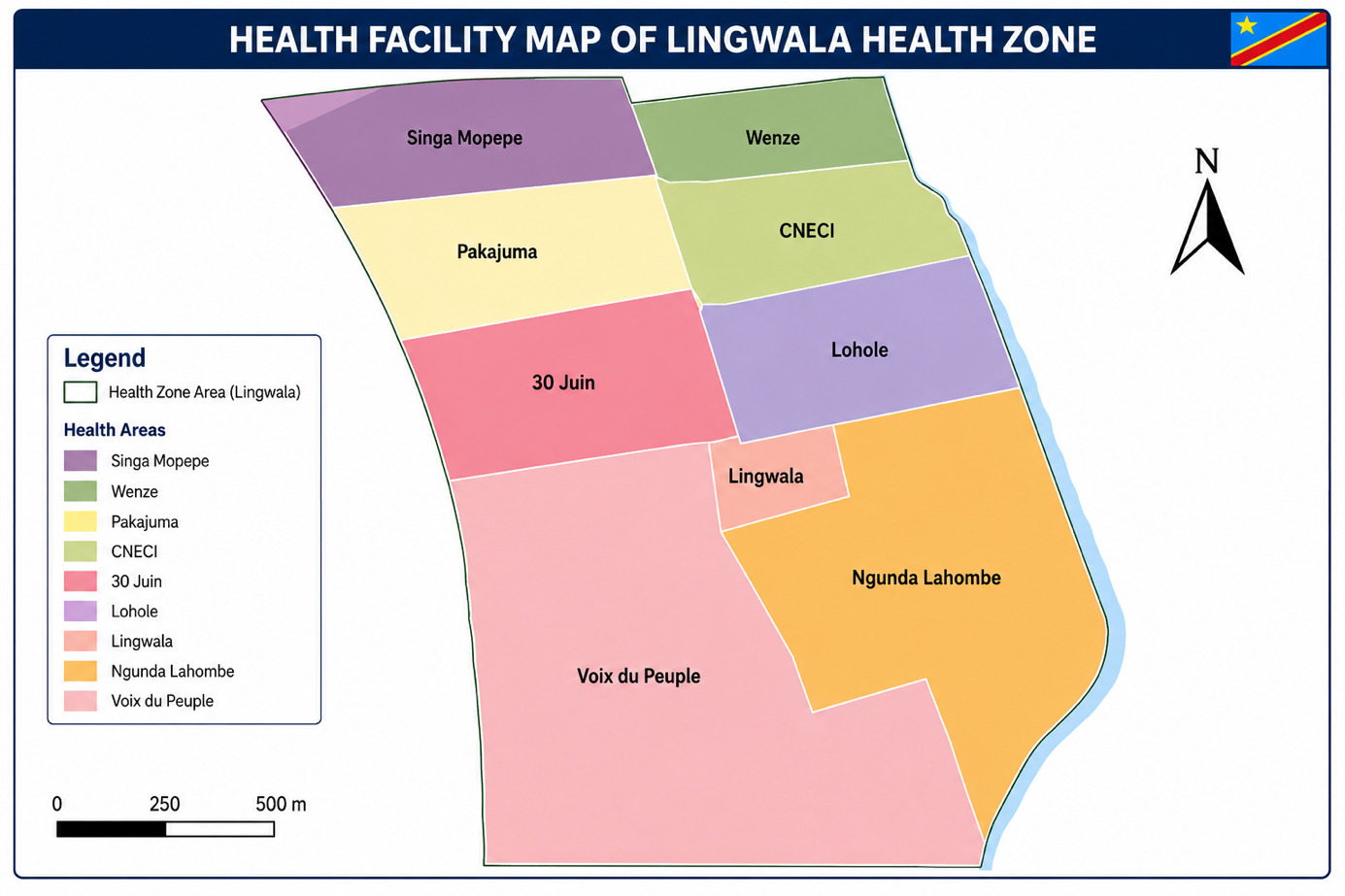
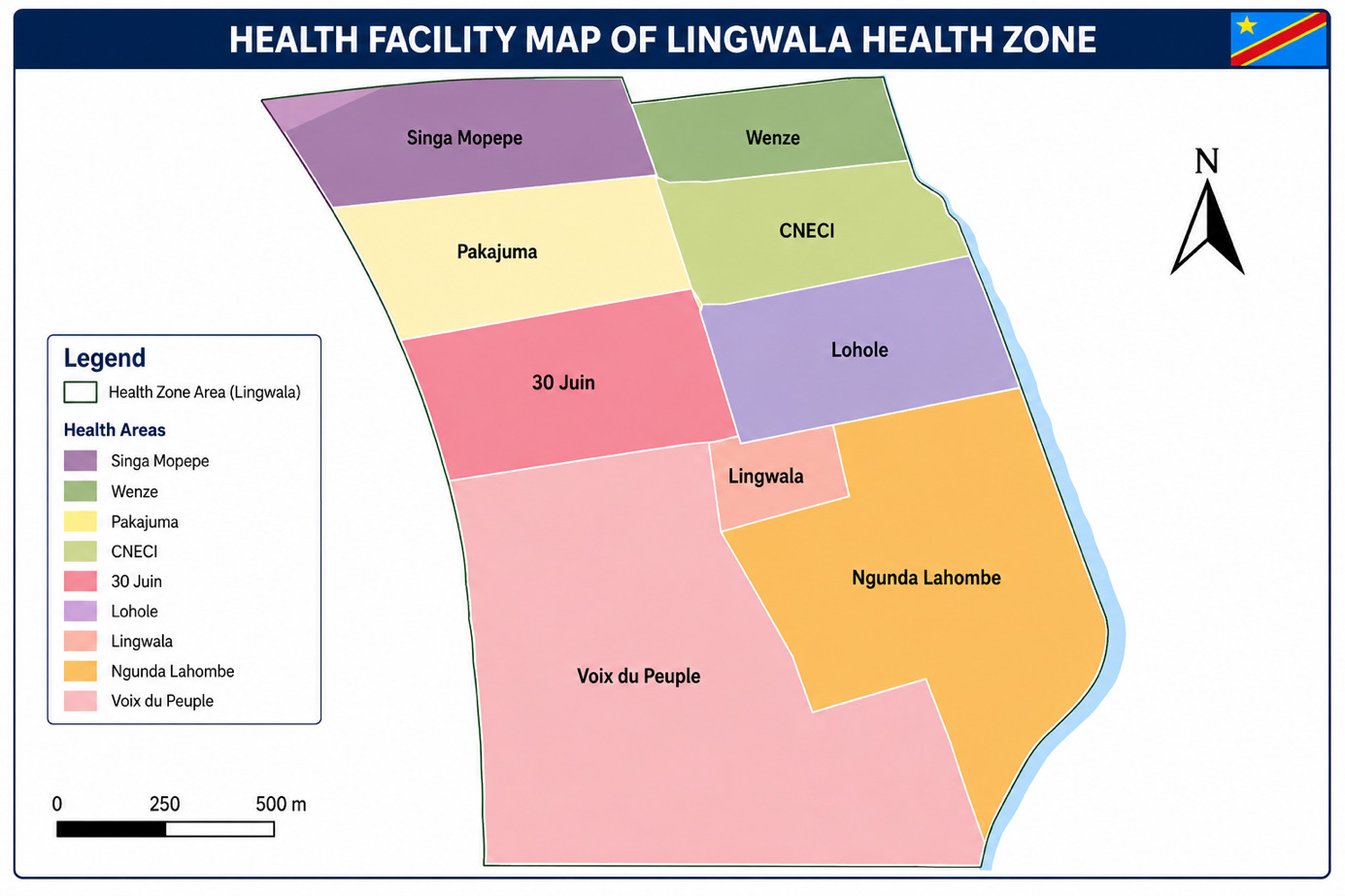
The study was conducted at the Diagnostic and Treatment Centre of Kabinda General Referral Hospital, located in the Lingwala Health Zone, Kinshasa, Democratic Republic of the Congo. In 2025, the Lingwala Health Zone had an estimated population of 284,728 inhabitants and covered an area of 2.9 km². It is bordered to the north by the Gombe Health Zone, to the south by the Kasa-Vubu Health Zone, to the east by the Kinshasa Health Zone, and to the west by the Gombe and Kokolo Health Zones.
The Lingwala Health Zone comprises eight health areas: La Voix du Peuple, Trente Juin, Ngunda Lohombe, Lohole, CNECI, Wenze, Pakadjuma, and Singa Mopepe. It also includes several public health facilities that manage severe respiratory infections and other conditions, including Vijana Hospital, Kabinda General Referral Hospital, Kalembelembe Hospital, and Kitega Health Centre.
The Diagnostic and Treatment Centre of Kabinda General Referral Hospital is one of the 143 tuberculosis diagnostic and treatment centres in Kinshasa. It was selected for this study because it is a referral facility that provides specialised tuberculosis care to patients from other health zones in Kinshasa and from other parts of the country. Figure 1 shows the health facility map of the Lingwala Health Zone.
Study design and period
This was a case-control study conducted among tuberculosis patients treated at the Diagnostic and Treatment Centre of Kabinda General Referral Hospital between 1 January 2016 and 31 December 2022.
Study population
The study population comprised tuberculosis patients aged 18 years or older who received treatment at the Diagnostic and Treatment Centre of Kabinda General Referral Hospital during the study period.
Cases were defined as tuberculosis patients aged 18 years or older who experienced failure of initial anti-tuberculosis treatment. Controls were defined as tuberculosis patients aged 18 years or older who were declared cured or who successfully completed treatment.
Inclusion and exclusion criteria
Cases were eligible if they were aged 18 years or older, had received initial anti-tuberculosis treatment at the Diagnostic and Treatment Centre of Kabinda General Referral Hospital during the study period, and had documented treatment failure.
Controls were eligible if they were aged 18 years or older, had received anti-tuberculosis treatment at the same centre during the study period, and were declared cured or had completed treatment successfully.
Patients with multidrug-resistant tuberculosis at baseline were excluded. Records that were incorrectly completed or had substantial missing data were also excluded.
Sample size
The sample size was calculated using StatCalc in Epi Info version 7, assuming a 95% confidence level and 80% power. The calculation was based on a previous study conducted in the DRC by Misombo-Kalabela et al.,9 in which treatment interruption was significantly associated with treatment failure among patients aged 18 years or older, with an odds ratio of 2.72. The assumed proportion of controls who had interrupted anti-tuberculosis treatment was 50%.
Two controls were selected for each case. The minimum sample size was 162 participants, comprising 54 cases and 108 controls. After allowing for a 10% non-response rate, the final target sample size was 178 participants: 59 cases and 119 controls.
Sampling procedure
A sampling frame was developed from records of all tuberculosis patients aged 18 years or older who received care at the centre between 2016 and 2022. For each patient, treatment outcome was recorded.
Cases were selected by systematic sampling from the list of patients with documented treatment failure. The list contained 300 eligible patients. Patients were arranged alphabetically and numbered from 1 to 300. Using a sampling interval of five, the first case was randomly selected from numbers one to five, after which subsequent cases were selected by adding the interval of five until the required number of cases was reached.
For each case, two controls were selected by systematic sampling from the list of tuberculosis patients who were declared cured or who completed treatment successfully.
Definition of treatment failure
Treatment failure was defined according to WHO operational criteria. A patient was considered to have failed anti-tuberculosis treatment if one or more of the following conditions occurred: persistent sputum smear or culture positivity at five months or later during treatment; failure of sputum conversion after the intensive phase of treatment; or clinical worsening, relapse, or reappearance of positive bacteriology after a period of negativity.10
Study variables
The dependent variable was failure of initial anti-tuberculosis treatment.
Independent variables included sociodemographic and economic characteristics, knowledge and practices related to tuberculosis, and clinical and biological characteristics. Sociodemographic and economic variables included sex, age, marital status, occupation, education level, household size, number of meals per day, and distance between the patient’s home and the diagnostic and treatment centre. Behavioural and treatment-related variables included medication regularity, treatment interruption, use of alternative treatments, adherence to directly observed treatment during the first two months, communication with healthcare staff, tobacco use, and alcohol consumption. Clinical and biological variables included history of tuberculosis, initial sputum smear result, clinical form of tuberculosis, sputum smear result after two months of treatment, HIV status, diabetes mellitus, other associated pathologies, and nutritional status.
Assessment of tuberculosis knowledge
Participants’ knowledge of tuberculosis was assessed using a composite score based on 10 binary items. Each item was scored 1 for “yes” and 0 for “no”. The questions were adapted from the PNLT PATI-6 tuberculosis management guideline on symptoms and clinical signs suggestive of tuberculosis.11 The total score ranged from 0 to 10. Knowledge was categorised as low knowledge for scores below 4, moderate knowledge for scores of 5–6, and high knowledge for scores above 6.
Data collection
Data were collected through document review and participant interviews. Clinical and biological data were extracted from diagnostic and treatment centre documents, including the treatment register, laboratory register, and individual patient treatment records. Sociodemographic data and information on tuberculosis knowledge, attitudes, and practices were collected through interviews with cases and controls.
Interviews were conducted either at the hospital or in participants’ homes, in a private setting to ensure confidentiality. The questionnaire was designed electronically and administered using KoboCollect version 3.4. Data-quality constraints were built into the electronic questionnaire to minimise entry errors.
Data analysis
Data were imported into SPSS version 25 for analysis. Categorical variables were summarised using frequencies and percentages. Quantitative variables were summarised using means and standard deviations for normally distributed variables, and medians with interquartile ranges for non-normally distributed variables. Normality was assessed using the Kolmogorov-Smirnov test.
Associations between treatment failure and sociodemographic, behavioural, clinical, and biological variables were assessed using logistic regression. Bivariable analyses were first conducted to estimate crude odds ratios and 95% confidence intervals. Variables considered clinically important or statistically associated with treatment failure in bivariable analysis were included in the multivariable logistic regression model. Potential confounders, including age, sex, and HIV status, were controlled for. Multicollinearity was assessed using the variance inflation factor, with values below 2 indicating no important multicollinearity. Model fit was assessed using the Hosmer-Lemeshow test. Statistical significance was set at p < 0.05.
Ethical considerations
The study protocol was reviewed and approved by the Ethics Committee of the School of Public Health, University of Kinshasa, under reference number ESP/CE/35/2024. Written informed consent was obtained from all participants before data collection. Confidentiality was maintained throughout the study, and all members of the research team were bound by professional secrecy regarding information collected from participants and patient records.
RESULTS
A total of 178 tuberculosis patients were included in the study: 59 cases and 119 controls. The results are presented according to sociodemographic characteristics, tuberculosis knowledge and practices, clinical and biological characteristics, and factors independently associated with failure of initial anti-tuberculosis treatment.
Sociodemographic factors associated with treatment failure
Table 2 shows the association between sociodemographic factors and failure of initial anti-tuberculosis treatment. In bivariable analysis, two sociodemographic factors were associated with treatment failure: consuming one meal or less per day and living far from the diagnostic and treatment centre. Patients who consumed one meal or less per day had markedly higher odds of treatment failure than those who consumed more than one meal per day. Patients who lived far from the diagnostic and treatment centre also had higher odds of treatment failure than those who lived nearer to the centre.
Knowledge, attitudes, and practices related to tuberculosis
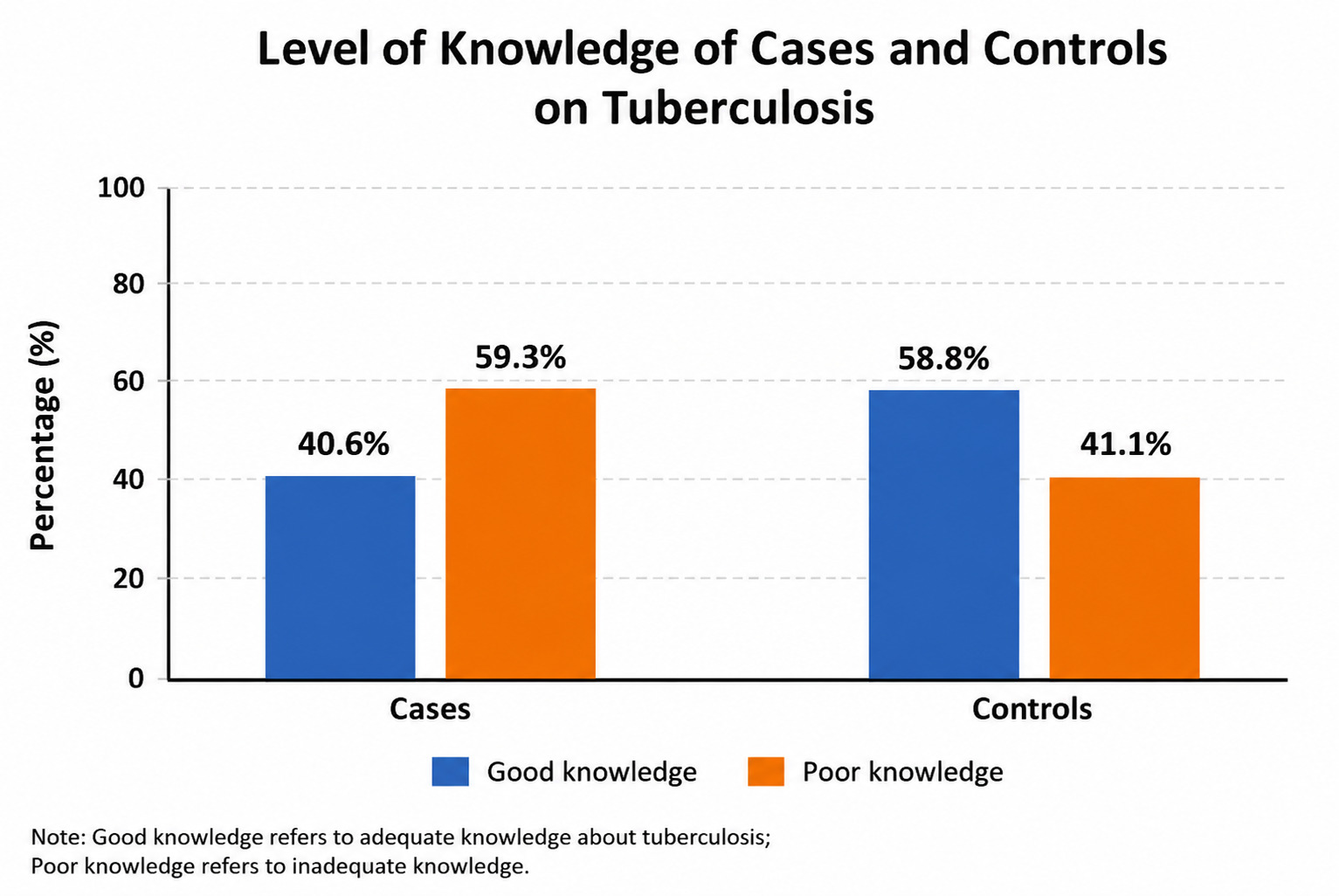
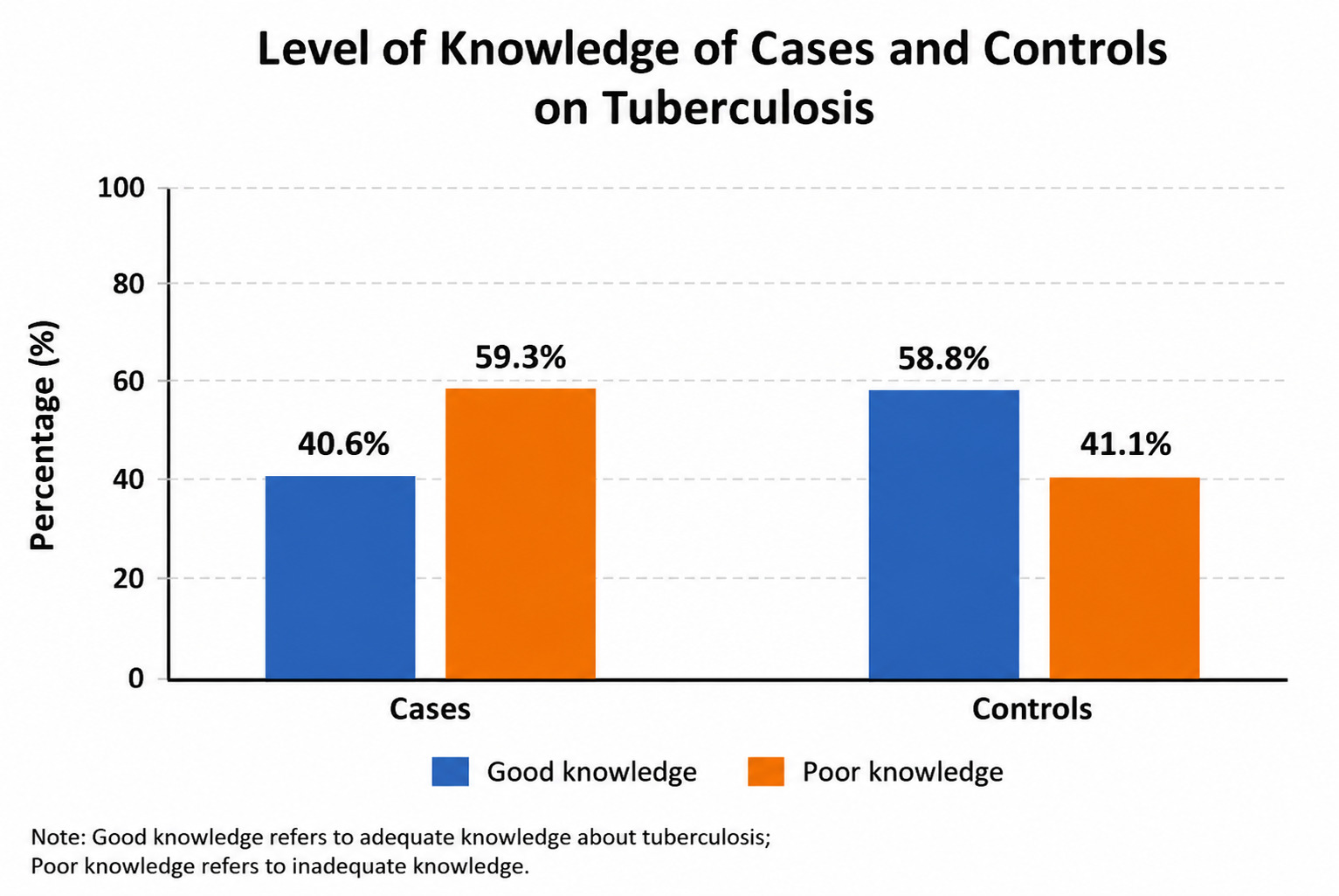
Table 3 shows the association between treatment failure and factors related to tuberculosis knowledge, attitudes, and practices. In bivariable analysis, irregular medication intake, use of alternative treatments during anti-tuberculosis treatment, treatment interruption, non-adherence to directly observed treatment during the first two months, and tobacco use were associated with treatment failure. Figure 2 shows the distribution of tuberculosis knowledge among cases and controls.
Clinical and biological factors associated with treatment failure
Table 4 shows the association between clinical and biological factors and failure of initial anti-tuberculosis treatment. In bivariable analysis, five factors were associated with treatment failure: history of tuberculosis, positive initial sputum smear, positive sputum smear at the second-month treatment follow-up, HIV-positive status, and diabetes mellitus. Positive sputum smear at the second-month follow-up showed the strongest association with treatment failure.
Factors independently associated with treatment failure
Table 5 presents the multivariable logistic regression model. Five factors remained independently associated with failure of initial anti-tuberculosis treatment: consuming one meal or less per day, irregular medication intake, non-adherence to directly observed treatment during the first two months of treatment, history of tuberculosis, and positive sputum smear at the second-month treatment follow-up.
DISCUSSION
This study assessed factors associated with failure of initial anti-tuberculosis treatment among patients followed at the Diagnostic and Treatment Centre of Kabinda General Referral Hospital in Kinshasa. A total of 178 participants were included, comprising 59 cases and 119 controls. The findings show that treatment failure was associated with socioeconomic vulnerability, treatment-related behaviours, and clinical and biological factors.
Men were slightly more represented among both cases and controls. This finding is consistent with evidence that tuberculosis notifications and disease burden are often higher among men than women in many low- and middle-income countries.12,13 This male predominance may reflect differences in exposure, healthcare-seeking behaviour, occupational risk, smoking, alcohol use, and other social or biological factors that influence tuberculosis risk and treatment outcomes.
Distance from the patient’s home to the diagnostic and treatment centre was associated with treatment failure in bivariable analysis, although this association did not remain statistically significant after adjustment. Similar findings have been reported in studies from Ethiopia and other sub-Saharan African settings.14–17 Long distance to care may increase transport costs, reduce attendance at follow-up visits, and contribute to missed drug-refill appointments. In low-income settings, these access barriers may compromise adherence to anti-tuberculosis treatment.
Consuming one meal or less per day was independently associated with treatment failure. Patients who consumed one meal or less per day had approximately ten times higher odds of treatment failure than those who consumed more than one meal per day. This finding is consistent with previous evidence indicating that poor nutritional status and food insecurity may negatively affect tuberculosis treatment outcomes.18 Tuberculosis and undernutrition are closely linked: tuberculosis can worsen nutritional status, while undernutrition weakens immunity and may impair recovery. These findings suggest that nutritional and socioeconomic support should be integrated into tuberculosis care, particularly for vulnerable patients.
Irregular intake of anti-tuberculosis medication was also independently associated with treatment failure. This is consistent with studies conducted in Kinshasa, Uganda, and Egypt.8,19,20 Irregular treatment may result from clinical improvement, return to work or other daily activities, medication side effects, poor counselling, transport barriers, or financial constraints. When patients feel better after the intensive phase, they may underestimate the importance of completing treatment. Strengthening adherence counselling, follow-up, and patient-centred support is therefore essential.
Treatment interruption was associated with failure in bivariable analysis, although the association did not remain statistically significant in the multivariable model. This finding is nevertheless important because treatment interruption is a recognised risk factor for poor outcomes, relapse, and drug resistance. Previous studies have reported strong associations between treatment interruption and failure.21 Intensified patient follow-up, home visits, community-based support, and early tracing of missed appointments may reduce treatment interruption and improve treatment success.
Non-adherence to directly observed treatment during the first two months was independently associated with treatment failure. This finding is consistent with earlier studies from Kinshasa and Uganda.9,22 The first two months of treatment represent the intensive phase, during which bacterial load is expected to decline substantially. Poor adherence during this period may delay sputum conversion and increase the risk of persistent infectiousness, treatment failure, and drug resistance. Directly observed treatment should therefore be strengthened, while ensuring that it is delivered in a patient-centred and non-stigmatising manner.
Tobacco use was associated with treatment failure in bivariable analysis but not clearly in multivariable analysis. Similar findings have been reported in studies from North Africa and other settings.23,24 Smoking may worsen lung damage, impair immune response, and reduce treatment effectiveness. However, tobacco use may be underreported because of stigma or social desirability bias. Tuberculosis programmes should include smoking cessation counselling as part of comprehensive patient care.
Alcohol use was not associated with treatment failure in this study. This finding is similar to a study conducted in Porto Alegre, where alcohol use was reported among patients with treatment failure but was not independently associated with failure.25 However, other studies have reported an association between alcohol use and poor tuberculosis treatment outcomes.26 The absence of an association in this study may reflect differences in measurement, underreporting, or limited statistical power.
Use of alternative treatments during anti-tuberculosis therapy was associated with treatment failure in bivariable analysis but not after adjustment. This differs from findings from Uganda, where concurrent use of other treatments was associated with anti-tuberculosis treatment failure.22 Alternative treatment use may delay care, interfere with adherence, or reflect dissatisfaction with biomedical treatment. Further qualitative research may help clarify why patients use alternative treatments during tuberculosis care.
In this study, the level of tuberculosis knowledge was not associated with treatment failure. Approximately 41% of cases had good tuberculosis knowledge, which was similar to the proportion among controls. This finding may suggest that knowledge alone is insufficient to ensure adherence and treatment success. Structural barriers, poverty, nutrition, access to care, and quality of follow-up may be more important determinants of treatment outcome in this setting. Similar findings have been reported in Tanzania,27 although other studies have found that poor tuberculosis knowledge is associated with treatment failure.21
History of tuberculosis was strongly associated with treatment failure. Patients with a previous history of tuberculosis had approximately twelve times higher odds of treatment failure. This association has been reported in previous studies from the DRC and other countries.9,16,28 Previous tuberculosis may reflect prior incomplete treatment, poor adherence, relapse, reinfection, or drug resistance. Patients with a history of tuberculosis should be considered at higher risk and should receive careful assessment, including molecular testing where available, to guide appropriate treatment.
Positive sputum smear at the second-month treatment follow-up was the strongest independent predictor of treatment failure. Patients with persistent smear positivity at two months had markedly higher odds of treatment failure. This finding is consistent with studies from the DRC, Benin, Nigeria, and other settings.8,29,30 Sputum smear conversion is an important indicator of treatment response. Persistent positivity may indicate high baseline bacillary load, poor adherence, drug resistance, or, in some cases, detection of non-viable bacilli. When sputum smear remains positive at the end of the second month, guidelines recommend close evaluation, adherence assessment, and extension of the intensive phase where appropriate.31
Tuberculosis/HIV coinfection was associated with treatment failure in bivariable analysis but not after adjustment. This finding is consistent with a previous study from the DRC in which HIV seropositivity was similar among cases and controls.8 However, studies from other sub-Saharan African countries have reported significant associations between tuberculosis/HIV coinfection and treatment failure.7,32,33 In this study setting, the presence of Médecins Sans Frontières at Kabinda General Referral Hospital, providing free care and nutritional support to patients with tuberculosis/HIV coinfection, may have reduced the adverse effect of HIV on treatment outcome.
Diabetes mellitus was associated with treatment failure in bivariable analysis but not in multivariable analysis. Similar findings have been reported in studies from Kinshasa.8,9 Diabetes may influence tuberculosis treatment outcomes through impaired immunity, delayed sputum conversion, and altered pharmacokinetics of tuberculosis drugs. Although the association did not remain statistically significant after adjustment, screening and management of diabetes among tuberculosis patients remain important.
Initial sputum smear positivity was associated with treatment failure in bivariable analysis but not after adjustment. Similarly, the clinical form of tuberculosis was not associated with treatment failure. This is consistent with evidence from Tunisia, where no association was found between clinical form and treatment failure.17 Nutritional status, measured as underweight, was also not significantly associated with treatment failure, although undernutrition remains clinically important in tuberculosis care. Previous studies have reported mixed findings regarding the association between low body weight and treatment failure.34,35
Strengths and limitations
This study has several strengths. First, it used a case-control design, which is appropriate for examining factors associated with relatively uncommon outcomes such as treatment failure. Second, data were obtained from both clinical records and participant interviews, allowing assessment of sociodemographic, behavioural, clinical, and biological factors. Third, interviews were conducted privately and separately to reduce contamination between participants and protect confidentiality.
However, the study also has limitations. Because of its observational design, causal relationships cannot be established. Some variables, particularly adherence behaviours, treatment interruption, tobacco use, alcohol use, and use of alternative treatments, may have been affected by recall bias or social desirability bias. The study did not include a qualitative component, which could have provided deeper understanding of the reasons for treatment interruption, poor adherence, or use of alternative care. Finally, some clinical and biological data depended on the completeness and accuracy of routine medical records.
Conclusions
This study identified factors associated with failure of initial anti-tuberculosis treatment at the Diagnostic and Treatment Centre of Kabinda General Referral Hospital in Kinshasa. Treatment failure was multifactorial and was associated with socioeconomic vulnerability, poor adherence to treatment, previous tuberculosis, and persistent sputum smear positivity after two months of treatment.
Five factors were independently associated with treatment failure: consuming one meal or less per day, irregular medication intake, non-adherence to directly observed treatment during the first two months, history of tuberculosis, and positive sputum smear at the second-month treatment follow-up.
These findings highlight the need for a comprehensive and patient-centred approach to tuberculosis care. In addition to ensuring access to effective medication, tuberculosis programmes should strengthen nutritional and socioeconomic support, adherence counselling, directly observed treatment, early follow-up of patients with missed appointments, and careful management of patients with previous tuberculosis or delayed sputum conversion. Such interventions could improve treatment success and reduce the risk of drug-resistant tuberculosis in the Democratic Republic of the Congo.
Funding
No funding was received for this study.
Authorship contributions
All authors contributed to the conception, design, conduct, analysis, interpretation, and writing of the study. All authors reviewed and approved the final manuscript.
Competing interests
The authors declare no competing interests.
Correspondence
Shadrak Kisalu Makaba
National Tuberculosis Programme
Democratic Republic of the Congo
Email: shadrakkisalu@gmail.com