Postnatal care (PNC) is a critical component of the maternal and newborn health continuum, encompassing care for women and newborns from immediately after birth up to six weeks (42 days) postpartum. This period is associated with heightened vulnerability to morbidity and mortality for both mother and child, making timely and adequate PNC essential for preventing avoidable complications and deaths.1
With an estimated 287,000 maternal deaths and 2.4 million newborn deaths each year, maternal and neonatal morbidity and mortality continue to be significant global public health issues.2 With maternal mortality rates above 500 per 100,000 live births and newborn mortality rates of over 27 per 1,000 live births, Sub-Saharan Africa and Southern Asia endure a disproportionate burden.3 Postpartum haemorrhage, sepsis, hypertensive disorders, preterm, and delivery asphyxia are the main causes of a significant percentage of these deaths, which happen in the early postnatal period. These illnesses are largely preventable with proper postnatal care.3–5 Research shows that over two-thirds of postnatal maternal deaths happen within the first week after delivery, and nearly half happen within the first 24 hours.6
The World Health Organisation (WHO) recommends structured postnatal care contacts, including an initial assessment within 24 hours of birth, followed by additional visits during the first six weeks postpartum.2 These visits provide opportunities for early detection and management of complications, promotion of breastfeeding, counselling on family planning, and support for maternal mental health. Despite these benefits, PNC remains one of the most neglected components of maternal health services in many low- and middle-income countries.
In Ethiopia, maternal mortality remains among the highest globally, with an estimated maternal mortality ratio of approximately 676 deaths per 100,000 live births.6 National coverage of postnatal care is particularly low, with fewer than one in ten women receiving any postnatal check within the recommended period.6,7 Although policy initiatives such as the Health Sector Development Programme and the Safe Motherhood (Making Pregnancy Safer) strategy emphasise a continuum of care, service utilisation remains suboptimal, particularly in rural and socioeconomically disadvantaged settings.4,5 Previous studies in Ethiopia have identified associations between PNC utilisation and factors such as maternal education, residence, income, place of delivery, antenatal care attendance, parity, and awareness of obstetric danger signs, with considerable variation across regions and communities.6,8
Understanding PNC utilisation requires a structured analytical framework. Andersen’s Behavioural Model of Health Services Utilisation conceptualises service use as the result of interactions between predisposing factors (e.g., age, education, marital status), enabling factors (e.g., income, residence, access to services), and need-related factors (e.g., obstetric history, perceived health needs).9,10 In addition, the Three Delays Model provides complementary insight by highlighting barriers related to decision-making, reaching health facilities, and receiving appropriate care. Together, these models offer a systematic approach to examining the multilevel determinants of postnatal care utilisation.
Despite growing literature on maternal health in Ethiopia, evidence on PNC utilisation in the Oromia region remains limited, and few studies explicitly link empirical findings to theoretically informed and policy-relevant strategies. Moreover, while descriptive studies have identified associated factors, there is limited clarity on how such evidence can be synthesised to inform practical, context-appropriate interventions.
Therefore, this study aimed to quantify postnatal care utilisation and identify factors associated with its use among postpartum women in Oromia, Ethiopia, and to formulate theoretically informed and expert-validated strategies to enhance PNC utilisation. By integrating empirical findings with established health service utilisation frameworks, the study aims to contribute evidence that informs maternal health planning and policy prioritisation in similar low-resource settings.
METHODS
Study design and setting
A facility-based cross-sectional quantitative study was conducted to examine postnatal care (PNC) utilisation and its associated factors and to inform the development of strategies to enhance PNC uptake among mothers in Oromia, Ethiopia. The study was guided by Andersen and Newman’s Health Services Utilisation Model and the Three Delays Model, which informed variable selection, analysis, and interpretation.
The Ambo General Hospital in central Oromia served as the study’s site. The hospital is a significant referral centre for the local rural and urban populations. With an estimated 83,053 residents and relatively decent access to healthcare and education, Ambo Town is a suitable place to examine differences in the use of maternal health services.
Study population, sample size, and sampling
The study population comprised postpartum women aged 18–49 years who had delivered within the preceding six weeks, regardless of whether they had utilised postnatal care services. Women were recruited while attending Ambo General Hospital for delivery-related care, newborn services, or postnatal follow-up during the data collection period. Participants were not selected based on prior PNC attendance, allowing for the estimation of utilisation prevalence and the identification of associated factors.
The sample size (n = 156) was determined using a single population proportion formula with a 95% confidence level, a 5% margin of error, and an estimated proportion of PNC utilisation drawn from previous studies, with adjustment for potential non-response. A sample size calculation was performed using Epi Info™, Version 7. Eligible participants were selected using a systematic approach based on daily attendance lists during the study period.
Data collection procedures and instruments
Data were collected using a structured, interviewer-administered questionnaire adapted from relevant literature and national maternal health survey tools. The questionnaire captured information on sociodemographic characteristics, obstetric history, health-seeking behaviours, knowledge and attitudes toward PNC, and health facility–related factors.
The instrument was translated from English into Afaan Oromo and back translated to ensure semantic consistency. The questionnaire was pretested among postpartum women in a comparable health facility, and minor revisions were made for clarity and cultural appropriateness. Data collectors received training on the study objectives, ethical considerations, and interview techniques, and field supervision was conducted throughout data collection to ensure data quality.
Study variables and theoretical framework
The primary outcome variable was PNC utilisation, defined as receipt of at least one postnatal care visit within six weeks of delivery. Independent variables were categorised according to Andersen’s model into predisposing factors (e.g., age, education, marital status), enabling factors (e.g., residence, income, distance to health facility, service cost), and need-related factors (e.g., obstetric history, antenatal care attendance, place of delivery).
The Three Delays Model was operationalised by mapping variables related to decision-making (e.g., education, attitudes), access (e.g., residence, transportation, distance), and service provision (e.g., cost, availability) to corresponding delays.
Data analysis
Epi InfoTM Version 7 was used for data entry, and SPSS Version 27 was used for analysis. To summarise participant characteristics and PNC use, descriptive statistics were employed. To investigate relationships between independent factors and PNC usage, bivariate analysis (chi-square tests) was carried out. To find independent predictors, variables with bivariate analysis p-values <0.25 were added to a multivariable logistic regression model.
95% confidence intervals (CIs) for adjusted odds ratios (AORs) were presented. Variance inflation factors were used to assess multicollinearity, and the Hosmer–Lemeshow goodness-of-fit test was employed to evaluate model fit. At p < 0.05, statistical significance was established. Statistically significant predictors were combined with constructs from Andersen’s Health Services utilisation Model and the Three Delays Model to create evidence-based strategies to improve PNC utilisation. A two-round Delphi technique, including experts in mother and child health, such as public health specialists, midwives, and health system managers, was then used to validate the draft solutions. A priori, consensus was regarded as ≥80% agreement among panellists.
Ethics considerations
Ethical approval was obtained from the University of South Africa Research Ethics Committee (Ref. No. 64111148_CRCE_CHS_2024) and the West Shewa Zonal Health Department. Written informed consent was obtained from all participants, who were informed of their right to withdraw at any time without consequence.
All data were de-identified prior to analysis, with unique study identification numbers replacing personal identifiers. Electronic data were stored on password-protected, encrypted computers, and hard-copy materials were kept in locked cabinets accessible only to the principal investigator. The study adhered to the ethical standards and data protection regulations of Ethiopia.
RESULTS
Sociodemographic characteristics
A total of 156 postpartum women participated in the study. The majority resided in rural areas (58%), while 42% were urban residents. Most participants were Oromo (65%), followed by Amhara (23%), with the remainder from other ethnic groups (12%). Most respondents were married, and nearly half (46%) reported a monthly household income of < ETB 3,000. Family size was relatively large, with 47% reporting five to seven household members. Overall, 43% of mothers demonstrated positive attitudes toward postnatal care (PNC), while 57% held negative perceptions.
Reproductive and obstetric characteristics
The mean age at first marriage was 21.0 ± 2.6 years, and 28% of women experienced their first pregnancy before the age of 19. Regarding obstetric history, 28% had one live birth, 37% had five or more pregnancies, and 35% reported five or more deliveries. Complications during labour were reported by 40% of respondents, while 13% experienced adverse obstetric outcomes. At the time of the survey, 29% of women were pregnant, of whom 5.7% reported the pregnancy as unintended.
Antenatal, delivery, and postnatal care utilisation
Antenatal care (ANC) utilisation was relatively high, with 62% of mothers attending at least one ANC visit and 36% completing four or more visits. However, PNC utilisation remained low at 31% (n = 48) within six weeks postpartum.
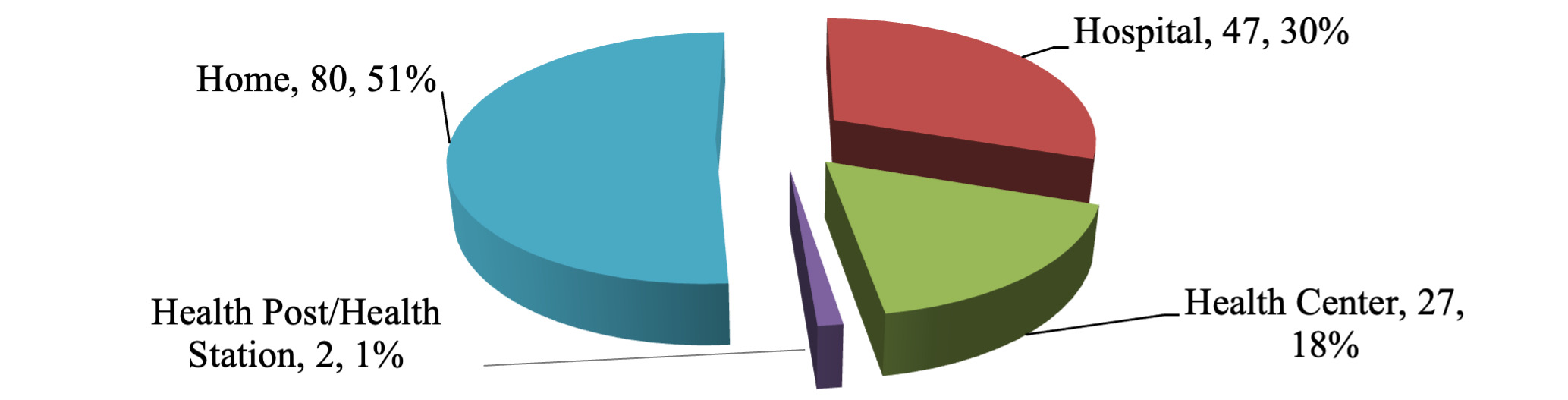
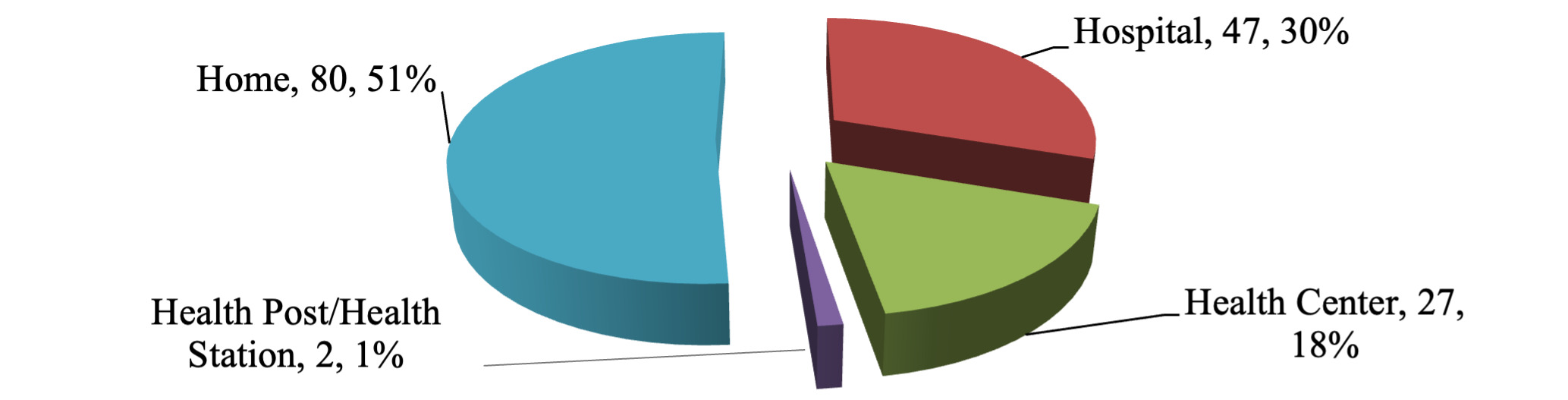
More than half of the respondents (51%, n = 80) gave birth to their most recent child at home. Among facility deliveries, 30% occurred in hospitals, 17% in health centres, and 1% in health posts. These results are detailed in Figure 1 & Table 1.
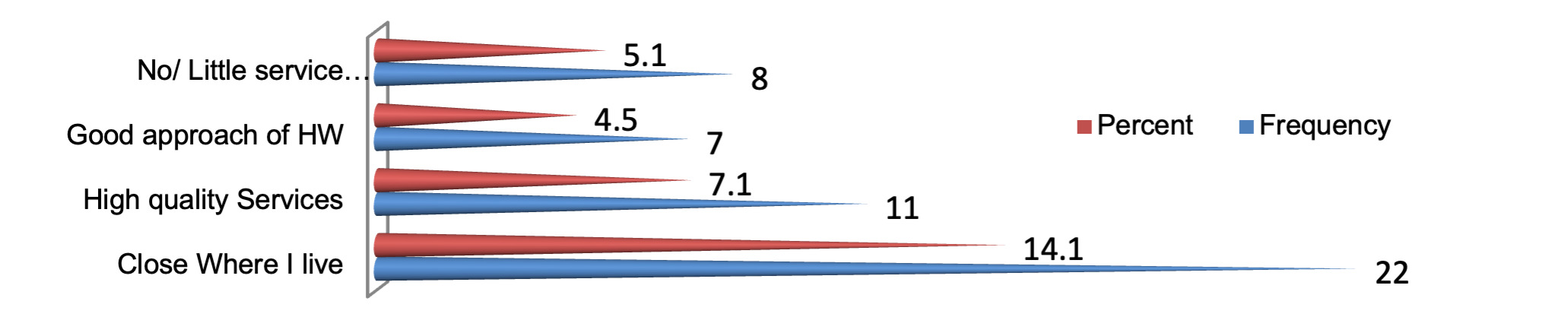
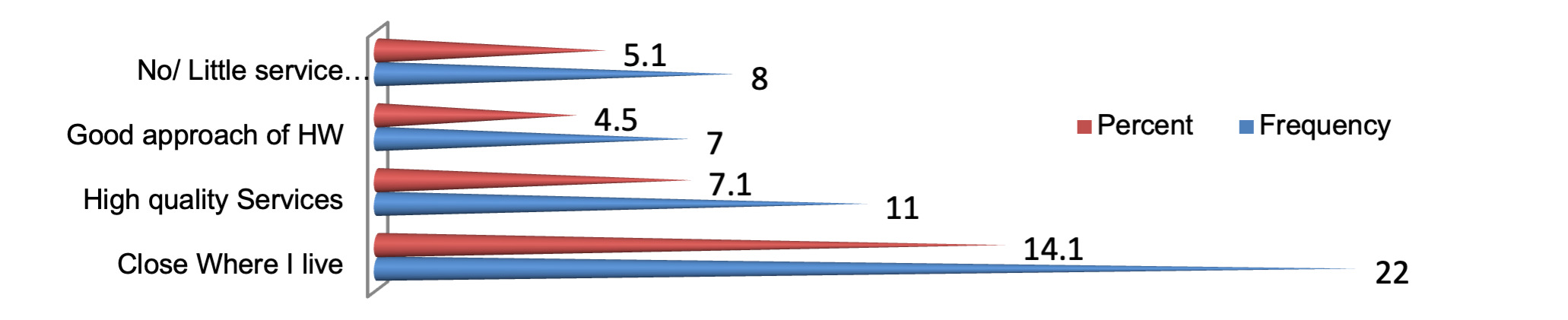
Overall, 49% of mothers delivered with the assistance of skilled birth attendants. The most commonly reported reasons for home delivery were perceived poor quality of services (23%), preference to stay with relatives (12%), and financial constraints (11%). In contrast, reasons for facility delivery included proximity to the facility (21%), perceived quality of care (13%), respectful approach by healthcare workers (8%), and minimal or no cost (4%). This is depicted in Figure 2.
Knowledge and attitudes related to maternal health
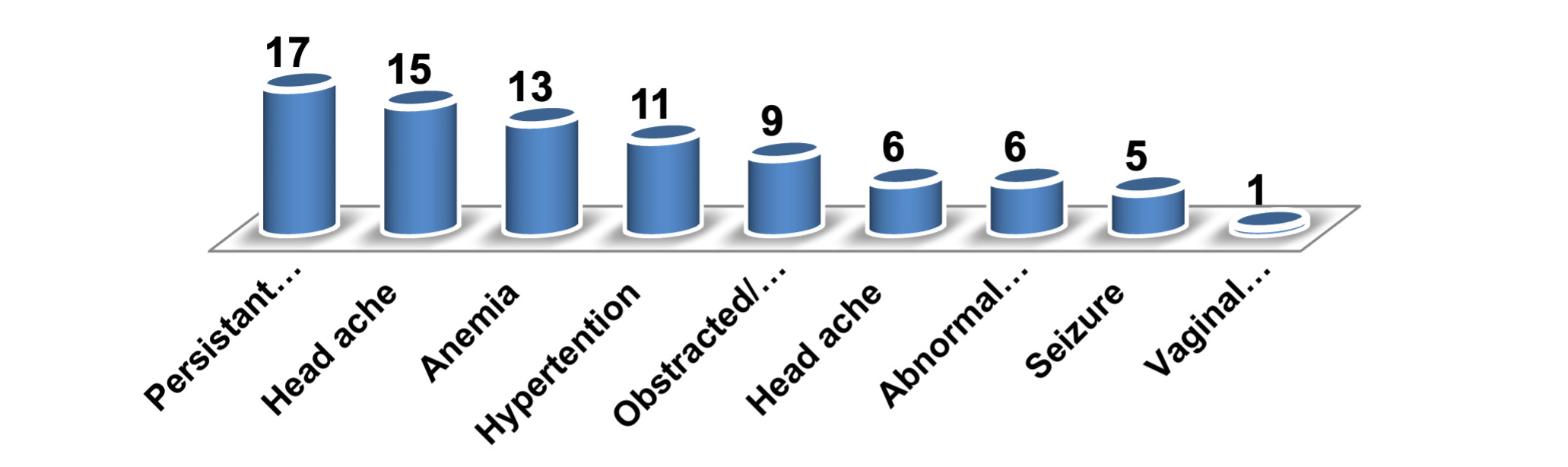
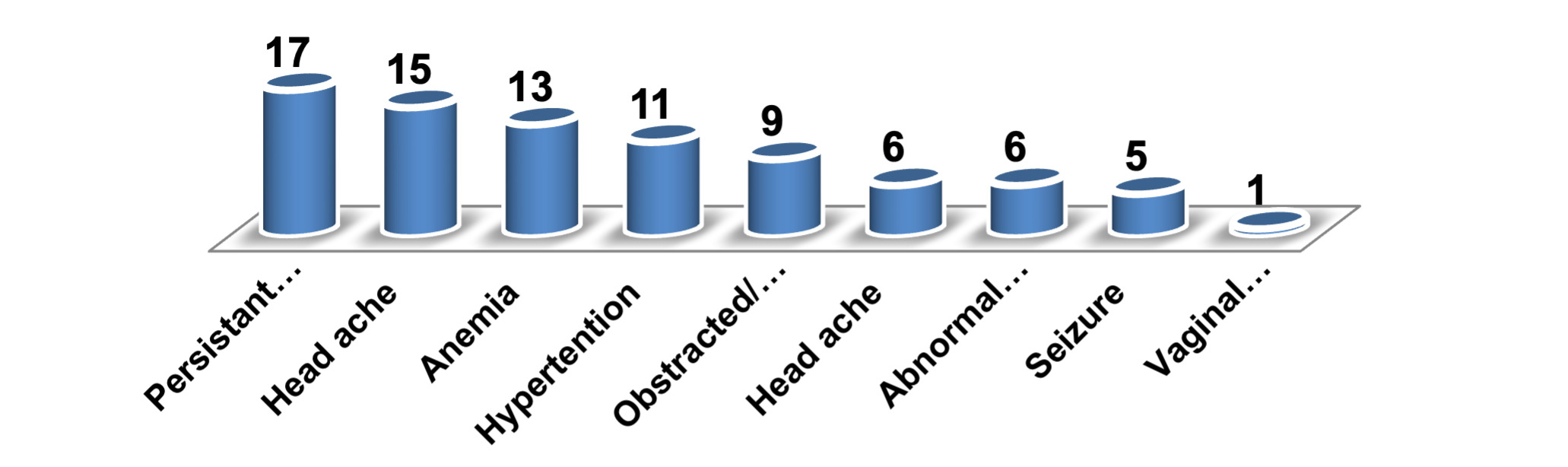
Over half of the mothers (53%) identified at least one danger sign during pregnancy, such as persistent vomiting, headache, or anaemia. (noted in Figure 3).
Knowledge of labour-related danger signs was reported by 51%, with prolonged labour, retained placenta, and malpresentation being the most frequently mentioned.
Although 85% of respondents expressed favourable attitudes toward managing pregnancy-related health risks and 52% supported facility-based delivery, this did not consistently translate into PNC utilisation, highlighting a gap between awareness and practice.
Access to and cost of services
Most respondents (79%) lived within one hour’s walking distance of a health facility, and 77% reported that their nearest facility provided delivery services. Nevertheless, 40% incurred out-of-pocket expenses for PNC and 25% for delivery-related care, often due to medication and supply costs from private vendors. Among PNC users, only 6.3% considered the costs affordable. The median reported PNC-related expenditure was ETB 195.65.
The most frequently cited reasons for non-utilisation of PNC were lack of awareness (22%), perception of being healthy (21%), and competing domestic responsibilities (12%).
Factors associated with pnc utilisation
Bivariate analysis indicated that PNC utilisation was significantly associated with residence, education, income, family size, ethnicity, and previous delivery experiences.
In multivariable logistic regression analysis, maternal education, household income, place of delivery, residence, and prior PNC or ANC use remained independently associated with PNC utilisation. Mothers with higher educational attainment and higher income levels were more likely to utilise PNC services. Facility-based delivery was associated with subsequent PNC use, whereas rural residence and larger family size were associated with lower utilisation (Table 2).
Strategy development based on empirical findings
Based on the quantitative findings and guided by the Andersen Health Services Utilisation Model and the Three Delays Model, four integrated strategies were developed and validated through expert consensus:
-
Raising public awareness and community empowerment to address delays in decision-making to seek care.
-
Improving access and affordability of PNC services, particularly for rural and low-income women.
-
Enhancing women’s socioeconomic empowerment to strengthen autonomy and capacity to seek care.
-
Addressing cultural barriers and engaging male partners and community leaders to support sustained PNC utilisation.
Together, these strategies directly target the structural, socioeconomic, and cultural barriers identified in the study and provide an evidence-informed framework for strengthening postnatal care utilisation in the Oromia region.
DISCUSSION
This study demonstrates that postnatal care (PNC) utilisation in Oromia remains low and is shaped by a combination of access-related, socioeconomic, and sociocultural factors, rather than a single barrier. Interpreted through Andersen and Newman’s Health Services Utilisation Model and the Three Delays Model,9,10 the findings indicate that constraints in deciding to seek care, reaching services, and receiving care after delivery jointly contribute to suboptimal PNC uptake.
Access-related factors were strongly associated with PNC utilisation. Mothers who delivered at home, lived in rural areas, or faced longer travel times were significantly less likely to use PNC services. These findings align with the second delay of the Three Delays Model—difficulty in reaching appropriate care.10 Similar barriers related to distance, transportation, and weak referral systems have been reported in West Shewa and other parts of Ethiopia.11–13 Strengthening primary-level facilities, improving referral linkages, and expanding outreach or mobile services have been shown to improve continuity of maternal care in comparable settings.14,15
Predisposing factors, particularly education and age, were associated with PNC utilisation, with younger and more educated women more likely to seek care. Although many respondents expressed favourable attitudes toward maternal health, this did not consistently translate into postnatal service use, suggesting gaps in awareness regarding the timing, purpose, and benefits of PNC. Similar findings have been reported elsewhere in Ethiopia and other low-income settings.7,16,17 Integrating targeted PNC education into antenatal care and community health programmes may help address the first delay—decision-making to seek care—by reinforcing the importance of postnatal follow-up.12,13
Household income and family size emerged as important enabling factors. Women from lower-income households and larger families were less likely to utilise PNC, highlighting financial and caregiving constraints that limit service uptake. These findings are consistent with Andersen’s model, which emphasises the role of enabling resources in healthcare utilisation.9 Evidence from Ethiopia and similar contexts indicates that reducing out-of-pocket costs and supporting women’s economic empowerment can improve maternal health service utilisation.14,18,19
Sociocultural characteristics, including marital status, ethnicity, and religious affiliation, showed associations with PNC utilisation, indicating that community norms and household decision-making dynamics influence care-seeking behaviour. Comparable studies have documented the influence of cultural beliefs, family support, and religious norms on maternal health service utilisation.15,20–26 Addressing these factors requires culturally sensitive engagement with families, male partners, and community and religious leaders to promote acceptance of postnatal care.13,14
The four strategies proposed—improving access, raising awareness, enhancing socioeconomic empowerment, and addressing cultural barriers—were derived by mapping empirically identified determinants to the Andersen and Three Delays frameworks9,10 and validated through expert consensus. These strategies should be interpreted as priority areas for policy and programme planning, rather than prescriptive solutions, as their feasibility and effectiveness were not empirically tested within this study.19,26–32
CONCLUSIONS
Postnatal care utilisation in the Oromia region remains suboptimal and is influenced by interconnected sociodemographic, economic, and sociocultural factors, as well as health system access constraints.6,7 Guided by established health service utilisation frameworks,9,10 this study identified key determinants of PNC use and formulated four expert-validated, evidence-informed strategies to address them. While these strategies provide a structured framework for strengthening postnatal care, further implementation and evaluation research is required to assess their practicality, acceptability, and impact across diverse settings.13,14,27
Acknowledgements
The authors sincerely thank all women who participated in this study for their time and valuable contributions. We also acknowledge the support provided by the West Shewa Zonal Health Department, Oromia Region, Ethiopia, and the staff of Ambo General Hospital for facilitating data collection. Special appreciation is extended to the supervisors, coaches, thesis advisers, and technical specialists at the University of South Africa (UNISA) for their guidance and support throughout the study.
Ethics Statement
Ethical approval for this study was obtained from the University of South Africa (UNISA) Research Ethics Committee (Ref. No. 64111148_CREC_CHS_2024) and the West Shewa Zonal Health Department, Ethiopia. Permission to conduct the study was obtained from the relevant gatekeeper institutions prior to data collection. Written informed consent was obtained from all participants. Confidentiality, privacy, and anonymity were maintained throughout the study, and all procedures were conducted in accordance with relevant ethical principles and guidelines.
Data Availability
The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request and subject to appropriate ethical and institutional approvals.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authorship Contributions
AAB contributed to the study conceptualisation, methodology, data collection, data analysis, interpretation of findings, manuscript drafting, and revision. RGM contributed to the study conceptualisation, methodology, supervision, critical review, and revision of the manuscript. MCM contributed to the study conceptualisation, methodology, supervision, critical review, and revision of the manuscript. All authors read and approved the final version of the manuscript.
Disclosure of Interest
The authors completed the ICMJE Disclosure of Interest Form and declare that they have no competing interests relevant to this study. The disclosure forms are available from the corresponding author upon reasonable request.
Additional Material
Materials describing the development and validation of the proposed postnatal care strategies are available from the corresponding author upon reasonable request.
Correspondence to:
Abate Argaw Buje
University of South Africa, Department of Health Studies, College of Human Sciences
1 Preller Street, Muckleneuk Campus, PO Box 392, South Africa, Pretoria, 0001
Email: abate.argaw@gmail.com / 64111148@mylife.unisa.ac.za